This is a story about medical notes...
My ex-wife - a biochemist by way of undergraduate degree - once screamed at me in an incoherent rage because I had innocently asked her "how big is a protein?" having wondered how many nanometers across, the average protein molecule measured. The sheer audacity of me asking such a question enraged her, perhaps because free thinking is expressly forbidden in an academic world which promotes rote-learning of facts and examinations graded to a marking scheme, ahead of learning.
(The answer, by the way, is roughly 3 nanometres in radius).
When I attempt to answer a difficult question, I sometimes pause and chuckle. "What is consciousness?" came one question. Although I was desperate to talk about weakly interacting subatomic particles, General Relativity and nuclear fusion, I somehow managed to constrain myself to a meaningless analogy, while keeping quiet about my "mind's eye" which could picture every piece of information that captured my entire existence, smeared out in a infinitely thin sphere at the event horizon of a singularity, across all meaningful spacetime for the entire universe that I will ever perceive, which would have been rather a mouthful to express.
Just as one may cram for an exam the night before, I've attempted to only ever amass the prerequisite knowledge that may be considered the minimum viable to navigate whatever situations I have had to endure to reach my goals. Education has never seemed like an end in and of itself, given that our understanding of the fundmental nature of reality is evolving, and the Standard Model of particle physics is rather long in the tooth. Although I find it quite delightful that there are quarks named strange, charm and beauty in the particle zoo, I would find it rather frustrating to dedicate years of my life, obtaining a degree and writing a thesis using tools which may soon look as clunky and outdated as Newton's inverse-square law of gravity.
The mathematicians will mock physics as simply being applied mathematics. The physicists will mock chemistry as simply being applied physics. The chemists will mock biology as simply being applied chemistry, and so on.
Computers are now capable of solving equations and modelling real-world phenomena, potentially making algebra and calculus into dying arts, along with handwriting and long-division. The Fractal Geometry of Nature has revealed that cold rational calculating machines can produce simulations that imitate reality, through repeating patterns. Massive computational power does not only aid human discovery of hidden algebraic equations.
Amid much fanfare, computer software is touted as potentiating new drug discovery by simulating molecular binding, protein folding, rapid gene sequencing and personalised medicine. However, we seem to have forgotten that half the planet is impoverished & hungry, and vast numbers of those who are fortunate enough to live in advanced, wealthy & technologically advanced societies, are suffering from an epidemic of anxiety, depression and other mental health issues that is bad enough to drive vast numbers of men in the prime of their life to commit suicide: the biggest killer of males under the age of 45 in the UK - more than road traffic accidents, drug-related deaths, physical disease, murder, accidents and all the other causes of death.
One should consider that I took leave of my senses in 2008, but since that time I have only managed to attract two clinical diagnoses - convenient medical short-hand - although I have acquired a third which is perhaps the bluntest instrument of the three, and much more of a pejorative than a diagnosis.
"Substance abuse" is a catch-all term which serves me well when I haven't the time & energy to go into detail. Given humanity's long history of self-intoxication, some physicians would consider themselves to be well-versed in the matter. Even the most insulated amongst us, will have struggled to escape contact with a drunk in our lives. We quickly forget, of course, that psychiatry is an extremely young discipline. The isolation, refinement and synthesis of molecules which can short-circuit brain mechanisms, is something that dates back only 70 or 80 years, along with the branch of medicine chiefly concerned with treatment of matters of the mind.
The brain: the most complicated organ in the human body - estimated to have up to a quadrillion neuronal synapses - is often considered only in terms of its vital function as central nervous system, insofar as the same fatty grey matter helps other species to fuck, fight, flee and feed. This does not, however, tell us much about human consciousness, and even less still about pathological thought.
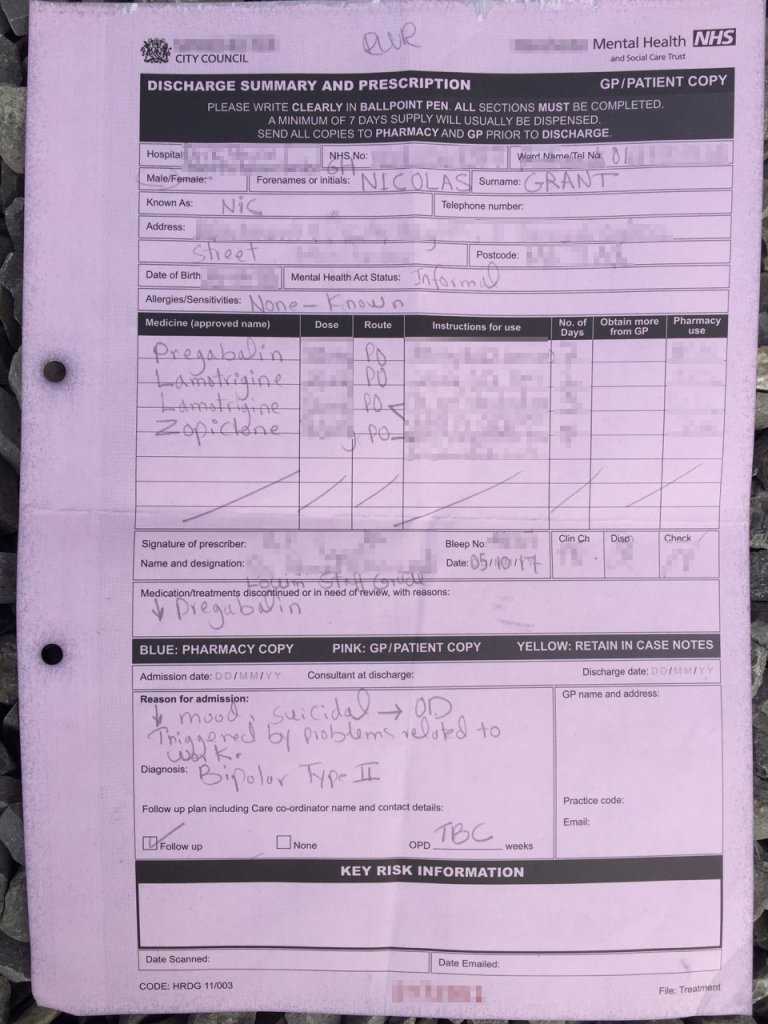
I once sat down and hand-wrote 12 pages of notes, from memory, of every General Practice doctor, psychiatrist and hospital, which I had attended during a 7 year period. Although I kept things as brief as I could, with names, dates and locations, as well as diagnoses and medications, there was a great deal to write. I'm not a complete hypochondriac - there were important notes about my episodes of depression and hypomania, where my mental health had caused me to become significantly dysfunctional.
Perhaps your mind is now skipping ahead - as mine often does - and you're attempting to finish my sentences. Presumably, you're trying to guess the punchline of the joke. I assume you've already got more than enough information to diagnose and treat me.
I'm second-guessing myself here, and I'm struck by the egotism and "navel gazing" of the very act of being sufficiently appraised of my own medical history that I should remember such a level of detail. Who the hell am I to take an interest in my own diagnosis and treatment? Where's my certificate, framed on the wall? Where's the photo of me wearing a mortar board & gown, and clutching a scroll of parchment with a red ribbon tied around it?
When I think about where I should spend my precious time and effort, I'm not motivated by the prospect of being an understudy to a failure. While psychiatry continues to produce dismal outcomes for humanity, in terms of the epidemic of mental health problems, addiction and general societal collapse under the weight of stress and burnout, I'm reluctant to follow in the path of those who are not succeeding in improving the human condition. It should however be noted that I do not for a single moment, criticise the well-meaning intent of those in the healthcare professions, nor do I mean to discredit the lifesaving work that takes place every single day.
The idea of using myself as a case study seems quite ridiculous, but one must consider that it would be unethical to - for example - risk a person's life when there is a treatment available that has been proven to be more effective than placebo.
With a sample size of one, perhaps nothing useful can be gleaned from my first-hand experiences, but I have attempted to corroborate my findings with other evidence wherever possible. I have deliberately avoided areas where another data point would make no difference: what use would it be if I too experienced anorgasmia as a result of SSRI medication, for example?
A great deal of our knowledge regarding the anatomy of the human brain has been gleaned from unethical experiments on unconsenting psychiatric patients - lobotomies, testing of medications and induced seizures. Animal studies have been gratuitously gruesome, with a great deal of unnecessary suffering inflicted upon primates. I'm not an anti-vivisection nutcase, but there must be very tangible goals to justify the means of obtaining the results.
To bathe a brain in psychoactive molecules that will cross the blood-brain barrier, is barbaric when we consider that the theoretical reasons why drugs have the effect that they do - the theories have so often been disproven. The 'chemical imbalance' theory that said that depressed brains had lower levels of serotonin, and that SSRIs would increase levels of synaptic serotonin, has been conclusively disproven, yet it is still a widely-circulated myth.
The much-vaunted sequencing of the human genome looks like a ridiculous white elephant of a project, when we consider that epigenetic gene expression had been discovered to allow genetically identical animals to exhibit completely different physical characteristics, depending on the environment that they have been exposed to.
In a collapsing global economy, education is one of the few sectors that's not feeling the pinch, and good solid science is getting drowned out in a sea of noise: pointless research. There are already excellent animal models which demonstrate that overpopulation and otherwise horrible living conditions, will produce a "behavioural sink" and addiction, in individuals who would otherwise lead happy healthy lives.
It has seemed fairly obvious to me from the start, that my mental health problems have stemmed from the ethical objections I had to the conduct of financial services organisations, and the role of global capitalism in ruining billions of human lives, in pursuit of unrestrained, unregulated and immoral profits, to the exclusion of any and all consideration of long-term consequences. In short: my problems should not be medicalised. I'm having a sane reaction to an insane world.
While this essay goes well beyond the "answer A, B or C" multiple-choice options on the prescriptive menu that is on offer, I feel that this does not invalidate the points I am making.
To have invested heavily in a mainstream education, would be to risk becoming incoherent with rage whenever somebody was so impertinent as to ask a thoughtful question - questions that spring into a mind that's unconstrained by the narrow status quo viewpoint, rote-learned while kowtowing to those with the necessary credentials to approve clones of themselves.
This is not "my ignorance is as good as your knowledge" anti-intellectualism, but instead a suggestion that we don't need so many people who've all read exactly the same books and sat more-or-less exactly the same tests. Moving towards intellectual homogeny is as dangerous as book burning, in my opinion.
In conclusion: this is a convoluted way of saying that you're unqualified to judge me, although you're possibly technically correct if you say that my problems are mostly of my own making.
Tags: #mentalhealth #suicide #addiction