This is a story about missed connections...
Like many people, I have a large collection of digital photos. My library starts in 2005, when a group of friends and I pooled our holiday snaps from a trip to Venezuela. Travel photography is the main thing that featured until my life started getting erratic. I have an increasingly random muddle of photos and screenshots, like a breadcrumb trail leading back to saner and more stable times.
2008 was the beginning of a much more exciting life than I had led before. I quit my investment banking career, developed some iPhone apps, retrained as an electrician, called off my wedding and went back to IT consultancy work. Having lived under the dark storm-cloud of an abusive relationship for far too long, I finally decided I'd had enough and broke up with my fiancée. I made a new group of friends and rebooted my life - as a prescription for depression, that shock treatment worked perfectly.
Fast-forward to 2011 and I knew that my relationship - back together with the girl who my friends call "the poison dwarf" - was destroying my world and ruining my happiness. I spent 3 amazing months in Cambridge and I'd fallen in love with somebody else, but I was too loyal; too faithful; too committed to give up on a failing relationship and go for what I really wanted.
In 2012 I capitulated and tried to follow doctor's orders - I started taking medication - and went back to the life I hated. I returned to the investment bank I'd previously worked for and tried to pretend like I was OK with that. I even got married to "the poison dwarf". I tried my very hardest to put on the boring grey suit and pretend like I was able to work doing the 9 to 5 office routine that I'd done for years and years, but my heart was broken.
I guess I never really got over the fact that I hadn't followed my dreams; followed my heart.
2013 brought the inevitable divorce, which necessitated selling my house and figuring out what to do with all my worldly possessions. In short, I didn't want anything to do with my toxic old life: the place and the things and the pain of everything getting ripped to shreds was just too much to bear. I wanted the whole lot to burn to the ground so I could start over. I wanted a fresh start.
I tried to court that girl from Cambridge who I'd fallen in love with - she liked me too and things were going well. It looked like I was going to break free from the gravity that tried to pull me back into a black hole. Despite me telling "the poison dwarf" that she could take as much as she wanted, she tried to destroy me. She just needed to leave me alone to get on with my new life, but she made the process of divorce into an unbelievably horrible disaster. Despite my attempts to make things quick and painless and give her a big cash settlement, she sabotaged my every effort.
In the midst of the acrimonious divorce, I tried to get away from the worsening British weather and get some rest and relaxation before Christmas. I was going to go to Florida and do some skydiving, and then I was going to go to San Francisco to see my friends in the Bay Area. The house should have been sold; the cash should have been in the bank - it wasn't, because "the poison dwarf" had screwed up the easy house sale that I'd worked so hard to make happen.
I was too sick to take my flight to America.
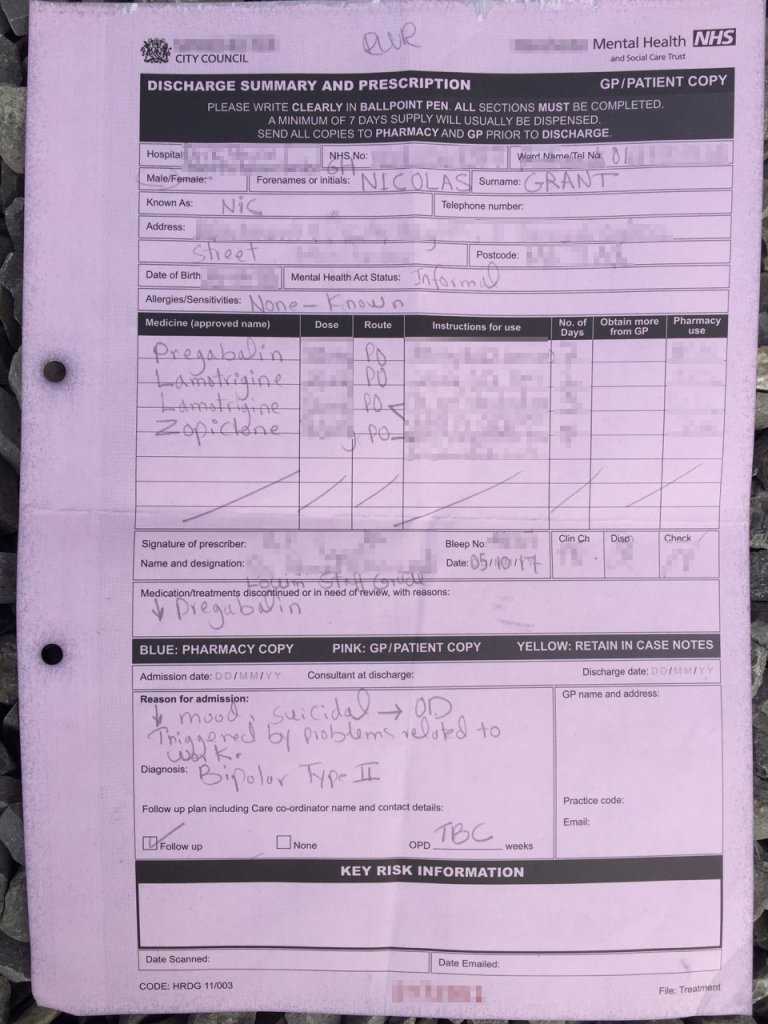
I think of 2014 as my annus horribilis given that I spent about 11 weeks receiving inpatient treatment, essentially for the problems caused by getting screwed over as a vulnerable person, by my ex-wife. She'd demanded a quick divorce and I'd said "take whatever you want" but then she made it unspeakably awful. After a rotten birthday where I found myself well and truly homeless, I repeated my magic trick of 2008: I got myself back into IT consultancy and made a load of new friends; I flew off to Tenerife with my new girlfriend and went kitesurfing. From the depths of despair and near destruction, I rose up and rebuilt myself.
What happened in 2015, 2016 and 2017, combined a winning formula of highly paid IT consultancy work and my ability to make new friends and rebuild my life, with the sensation-seeking desire to maintain a novel lifestyle: if nothing else, my life has been very exciting for the past few years.
Whereas most people live in fear of tarnishing their professional reputation and losing everything they own and hold dear, I found those things became incredibly cumbersome when I was unwell. To maintain appearances and pretend like everything is just fine, is immensely energy-draining. It's almost driven me insane, worrying about what former work colleagues and bosses think about me; what people know about my chequered past. Far, far, far more than the abuse my body has suffered, and the mental health problems I've been through, the biggest problem in my life has been worrying about people finding out the very things that I've catalogued on the pages of this blog, quite publicly.
We are now approaching a third San Francisco flight that has been booked, but there is a great deal of uncertainty regarding whether I will be going or not. I dearly wish to see an old schoolfriend who was pivotal in raising the alarm on social media, to the fact that I was in the process of killing myself - in essence, he was the last person I spoke to while still alive, telling him that I was sorry I wouldn't be seeing him in November [because I'd be dead].
It fucking horrifies me that the managing director of the company who I was working for at the time - who booked my flights out to San Francisco - was in the process of attempting to terminate my employment while I was on life support in intensive care... because he'd read this on Twitter!
Given that I've stubbornly refused to die, I feel like taking the trip to San Francisco in defiance of the arsehole who didn't care whether I lived or died. That gobsmackingly awful human being deserves to have to see me alive and well, taking a trans-Atlantic flight to go and see an old friend who actually cared about my life.
I feel like I might be calling on you - my social media friends - to help me raise Hell to show that vulnerable people shouldn't get screwed over by unscrupulous arseholes.
So, this is my call to action: I'd like to speak to you and I'd like your support in turning up the heat on people who put personal profit ahead of human lives. I've been wondering what to do with myself, and this feels like an important point; this feels like something symbolic.
Whether it's my ex-wife who literally said "I'd rather be a widow than a divorcee" or my ex-boss who literally fired me for being dead, I want to stand up to these fucking arseholes.
Tags: #career